Notes: The following information is intended for health care professionals. Always read the label and follow the instructions for use. For information on the efficacy and the side effects, refer to the instructions for use. Products are only for sale to health professionals.
What is Patient Registration?
Computer navigation systems are considered imageless or image-based, depending (as the name suggests) on whether they rely on imaging. Whereas an image-based system can use an image to measure a component’s position relative to patient anatomy, an imageless system does not have this direct information. Instead, the set-up process for an imageless system includes “patient registration”. The device “registers” a 3D pelvic coordinate system based on the patient’s rigid anatomy. This coordinate system locates the patient in 3D space and provides a reference frame, against which component orientations can be measured and reported.
What are the Types of Patient Registration?
Anatomical Landmarking
For most imageless computer navigation systems, the surgeon locates bony landmarks during the patient registration process. Many navigated surgeries rely on accurately palpating three bony landmarks: the anterosuperior iliac spines (ASISs) and the pubic symphysis1-6.

Table Tilt Method
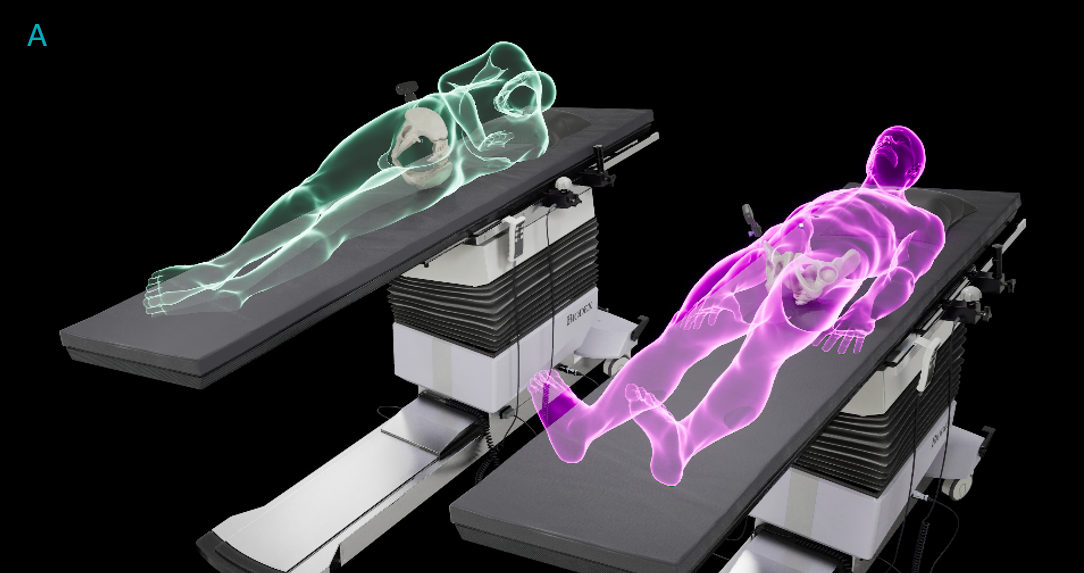
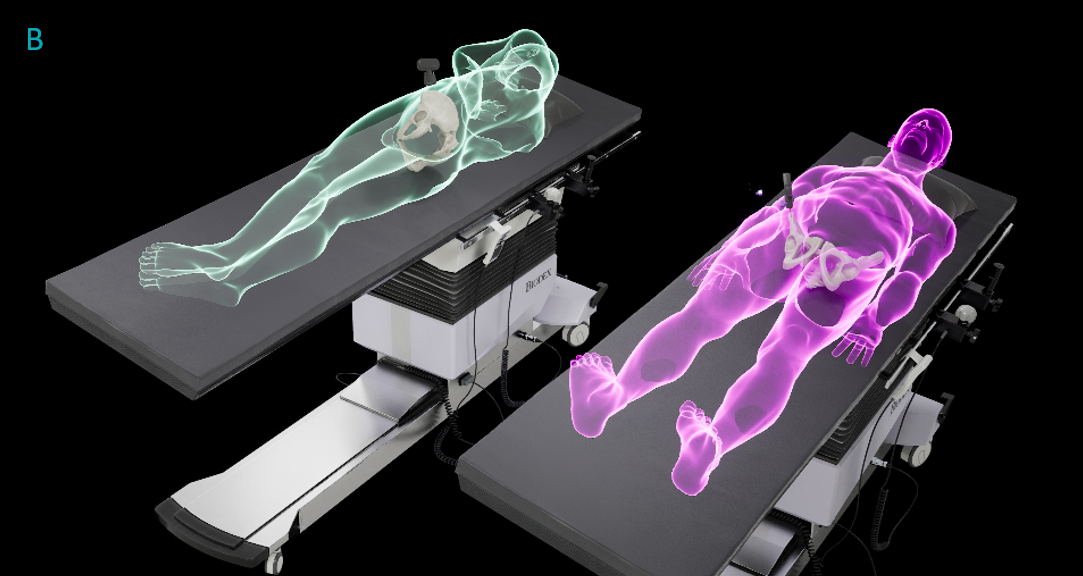
The Navbit Sprint System does not use anatomical landmarks for patient registration. Instead, the patient is aligned on the operating table, which is then tilted approximately 10° to the left (A) and right (B) during registration, guided by the device7. This table tilt method of registration relies on the correct alignment of the patient on the operating table, rather than the accurate identification of bony landmarks.
Does Accuracy Depend on the Type of Patient Registration?
In a word: yes.
In a recent study8, we compared the clinical accuracy of three methods concurrently. Two methods used landmarking during registration (ASIS Anatomic, ASIS Functional) and one used the table tilt registration method (TT Functional). Two methods used functional reference planes (ASIS Functional, TT Functional) and one used an anatomic reference plane (ASIS Anatomic). All measurements of acetabular cup inclination and anteversion were compared with the measurements from postoperative computed tomography (CT) scans. For inclination, the mean absolute error was significantly lower for both functional reference planes than for the anatomic reference plane (3.75°, p < .001). Additionally, inclination using the TT Functional method had significantly lower error (1.80°) than using the ASIS functional method, (2.74°), p = .038, although this difference was clinically small. For anteversion, the mean absolute error was significantly lower for both functional reference planes than for the anatomic reference plane (8.58°, p < .001). These findings suggest that using functional reference planes leads to more accurate measurements of the acetabular cup position than using anatomic reference planes. The results also suggest that the table tilt registration method is able to achieve similar accuracy to using landmarks for registration.
How does the Table Tilt Method Achieve its Accuracy?
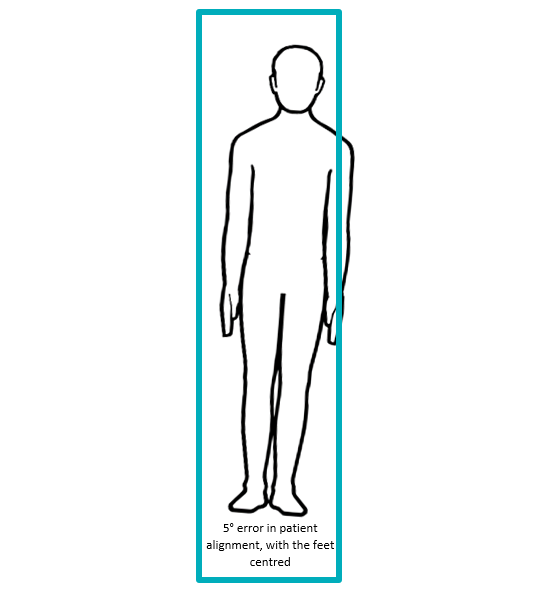
It is perhaps counterintuitive that aligning a patient on an operating table would be as accurate as a surgeon locating a bony feature. However, because both the patient and the table are long relative to their width, even a 5° error in patient alignment is visually evident to the surgical team, illustrated below. Such noticeability of alignment errors may support accuracy. We have previously discussed that identifying anatomic landmarks is prone to errors, particularly for anteversion, for a number of reasons. Both registration methods, therefore, have different sources of errors, but achieve comparable accuracy results.
Summary
In one clinical study, using functional reference planes resulted in significantly lower errors than an anatomic reference plane. The table tilt method of registration achieved similar accuracy to a landmarking registration method.
References
- Gurgel HMCP, Croci ATP, Cabrita HABAP, et al. Acetabular Component Positioning in Total Hip Arthroplasty With and Without a Computer-Assisted System – A Prospective, Randomized and Controlled Study. J Arthroplasty 2014;29(1):167-71. doi: 10.1016/j.arth.2013.04.017
- Davis ET, Schubert M, Wegner M, et al. A new method of registration in navigated hip arthroplasty without the need to register the anterior pelvic plane. J Arthroplasty 2015;30(1):55-60. doi: 10.1016/j.arth.2014.08.026 [published Online First: 2014/10/15]
- Lass R, Kubista B, Olischar B, et al. Total Hip Arthroplasty Using Imageless Computer-Assisted Hip Navigation A Prospective Randomized Study. J Arthroplasty 2014;29(4):786-91. doi: 10.1016/j.arth.2013.08.020
- Sendtner E, Schuster T, Wörner M, et al. Accuracy of acetabular cup placement in computer-assisted, minimally-invasive THR in a lateral decubitus position. Int Orthop 2011;35(6):809-15. doi: 10.1007/s00264-010-1042-4
- Cross MB, Schwarzkopf R, Miller TT, et al. Improving registration accuracy during total hip arthroplasty: a cadaver study of a new, 3-D mini-optical navigation system. Hip Int 2018;28(1):33-39. doi: 10.5301/hipint.5000533
- Wan Z, Malik A, Jaramaz B, et al. Imaging and Navigation Measurement of Acetabular Component Position in THA. Clin Orthop Relat Res 2009;467(1):32-42. doi: 10.1007/s11999-008-0597-5
- Shatrov J, Marsden-Jones D, Lyons M, et al. Improving Acetabular Component Positioning in Total Hip Arthroplasty: A Cadaveric Study of an Inertial Navigation Tool and a Novel Registration Method. HSS Journal® 2021;0(0):15563316211051727. doi: 10.1177/15563316211051727
- Farey J, Chai Y, Xu J, et al. Evaluating alternative registration planes for imageless, computer-assisted navigation during supine total hip arthroplasty. Orthopaedic Proceedings 2021;103-B(SUPP_14):9-9. doi: 10.1302/1358-992X.2021.14.009