Allowing for Pelvic Tilt in Supine Total Hip Arthroplasty (THA)
Using an adjusted intraoperative target, an estimated 99.7% of patients will be within ±10° of both the inclination and anteversion targets.

Using an adjusted intraoperative target, an estimated 99.7% of patients will be within ±10° of both the inclination and anteversion targets.
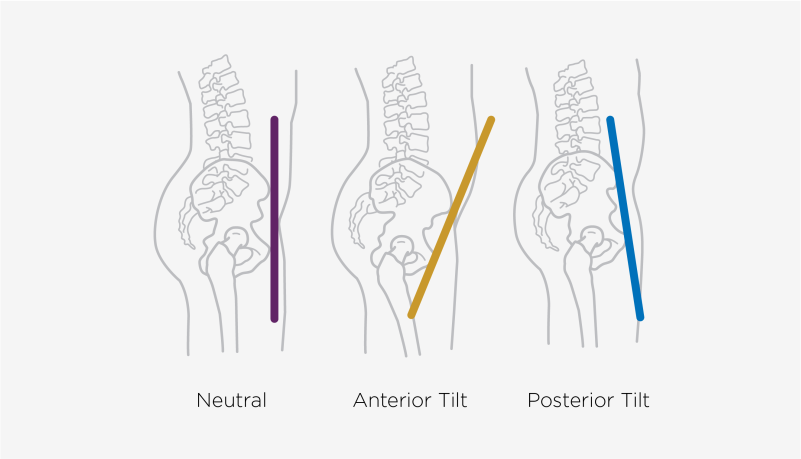
Pelvic tilt varies between the standing and supine patient positions 1, 2. With surgery in the supine position and the target acetabular cup orientation in the standing position, this raises a question: To achieve the target acetabular cup position, is there a need to assess the supine-to-standing pelvic tilt pre-operatively and to create a patient-specific plan?
In the present article, we conclude that a simple adjustment of the intraoperative target removes the need for complex, costly pre-operative planning. With an intraoperative target of 39° inclination and 16° anteversion, an estimated 99.7% of patients will be within ±10° of both the inclination and anteversion targets.

The pelvis typically tilts between the supine and standing positions. The average patient has 5.5 degrees of posterior pelvic tilt when they go from supine to standing 1, 2. Pelvic tilt is illustrated in Figure 1 and Figure 2.
Note: Adapted from Haffer, et al.
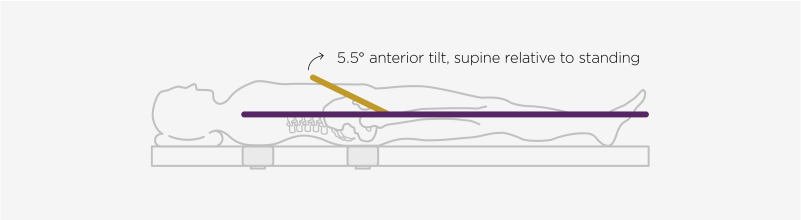
Note: Adapted from Wan, et al.
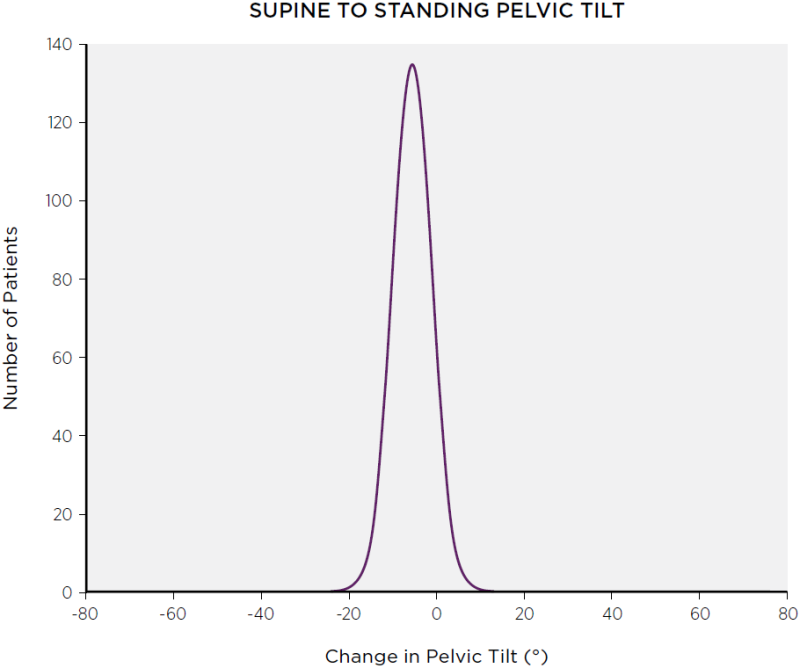
There is also variation in pelvic tilt between patients. Figure 3 shows the supine and standing pelvic tilts for 1517 patients in a study by Pierrepont, et al. 2. For the same group, the differences in tilt between standing and supine are shown in Figure 4. Both plots were approximated by the normal distributions that fit the figures in Pierrepont, et al. 2.
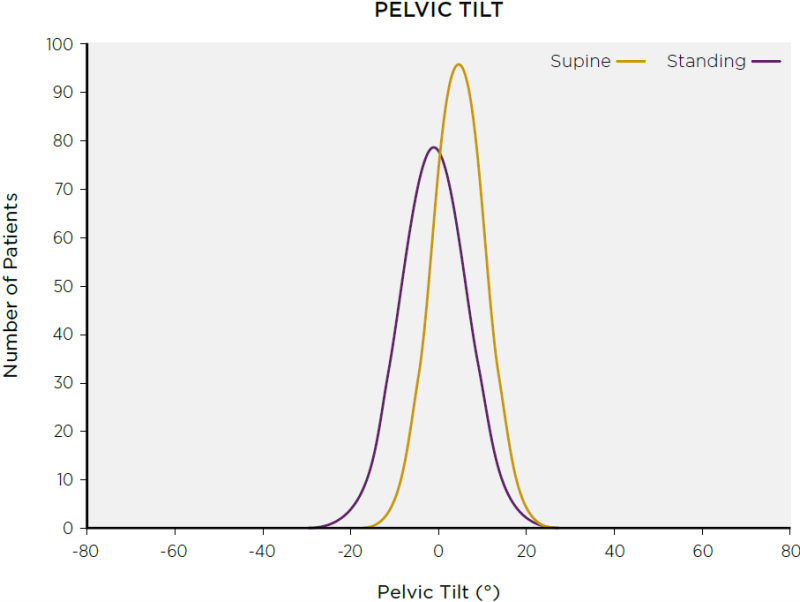 Note: Data were estimated based on Pierrepont, et al. 2.
Note: Data were estimated based on Pierrepont, et al. 2.
 Note: Data were estimated based on Pierrepont, et al. 2.
Note: Data were estimated based on Pierrepont, et al. 2.
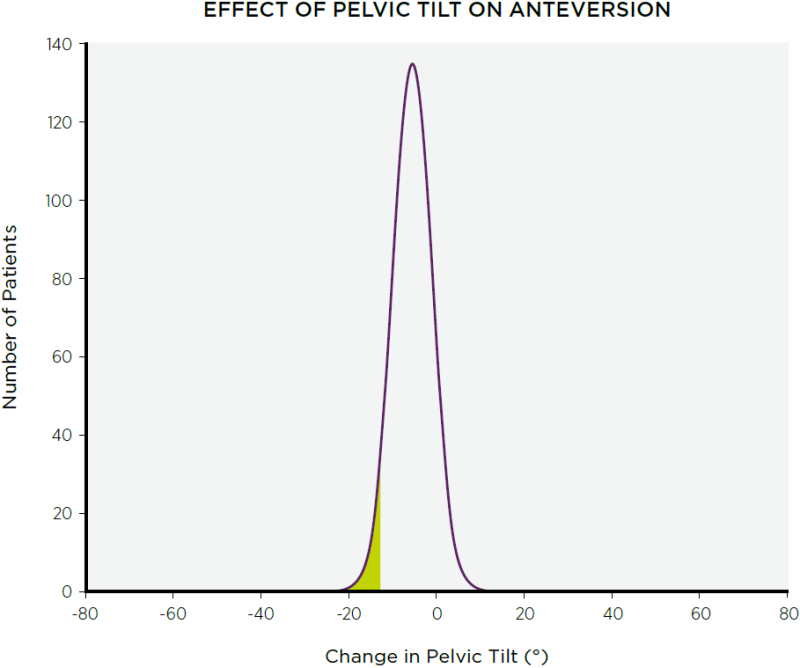
A concern in the literature is the effect on post-operative anteversion of this supine-to-standing pelvic tilt. This effect can be calculated using the definitions in Murray 5. Using the online calculator shown in Figure 5, a relative posterior change in pelvic tilt of 13° from supine to standing would increase the anteversion of the acetabular cup by 10°. Pierrepont, et al. 2 argued that, as a result, 6% of patients would have unacceptably high anteversion, shown in Figure 6. Their ensuing conclusion was that patient-specific planning is necessary prior to THA. However, such planning would add a significant burden of time, cost, complexity, and radiation. A simple alternative is available.
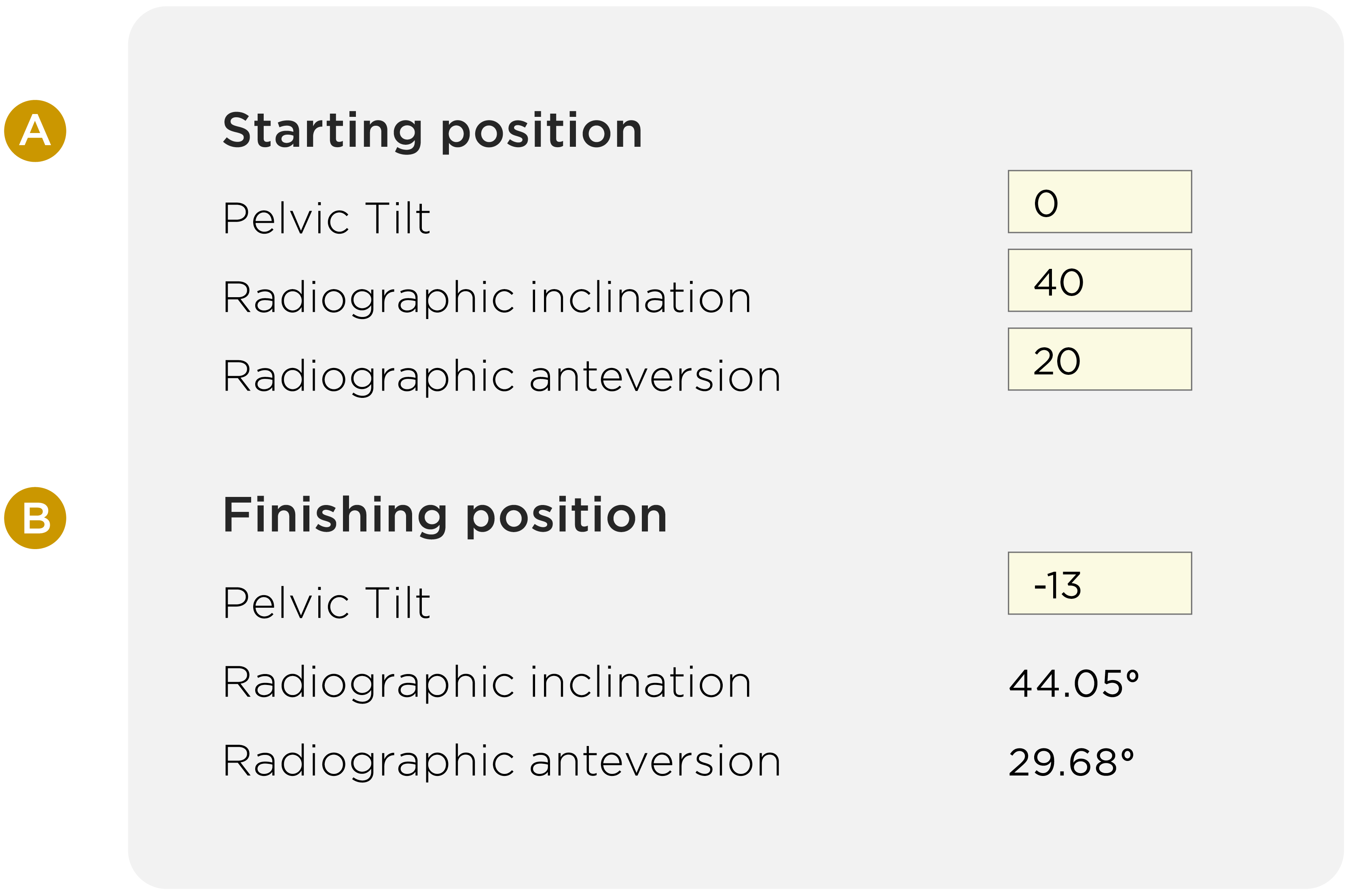 Note: The intraoperative (supine) target (A) results in the post-operative (standing) outcome, based on a 13° posterior tilt in standing relative to supine (negative is posterior). The calculator is available at http://billwalter.com.au/calculator/pelvic-tilt/
Note: The intraoperative (supine) target (A) results in the post-operative (standing) outcome, based on a 13° posterior tilt in standing relative to supine (negative is posterior). The calculator is available at http://billwalter.com.au/calculator/pelvic-tilt/
It is possible to adjust the intraoperative (supine) target for acetabular cup position so that the average patient has a 40°/20° post-operative (standing) cup position. With no adjustment (i.e. an intraoperative target of 40°/20°), the average patient tilt (-5.5°) has a projected post-operative acetabular cup position of 41°/24°. For this average patient, adjusting the intraoperative acetabular cup target to 39°/16° leads to a predicted post-operative acetabular cup position of 40°/20°, shown in Figure 7. Thus, the 39°/16° target achieves the desired outcome for the average patient.
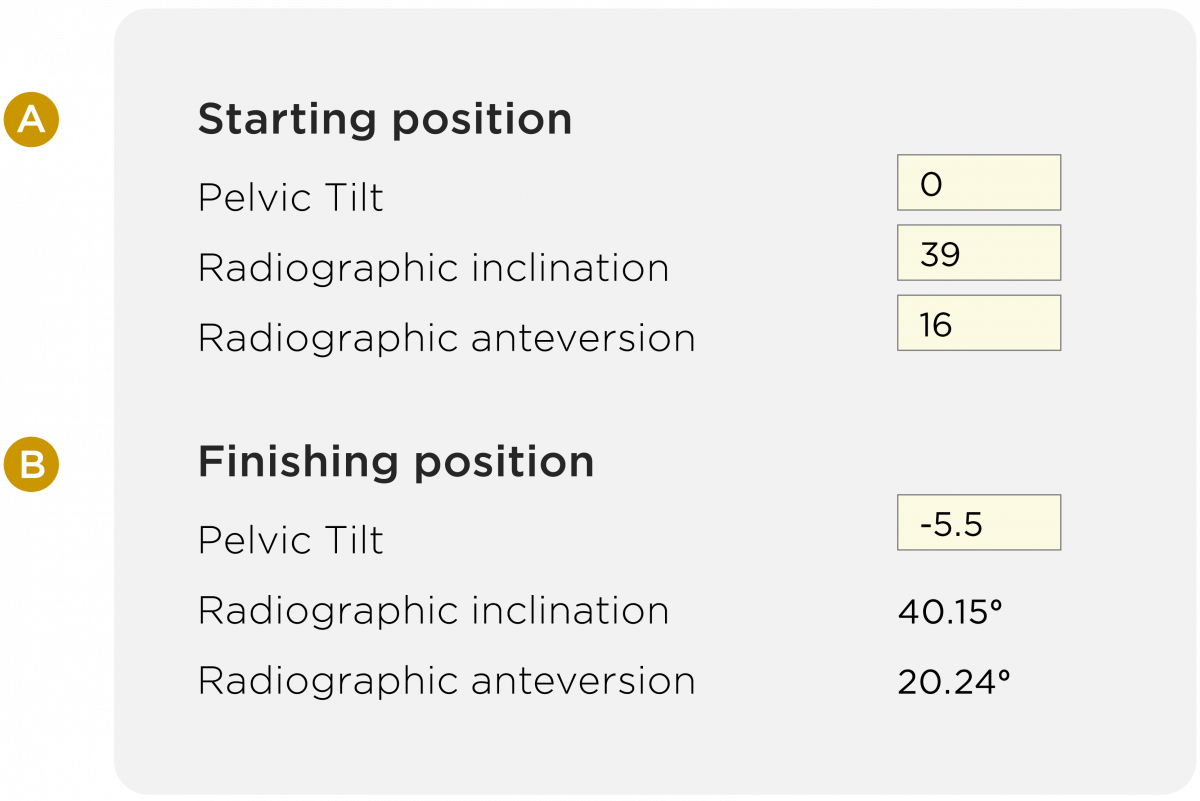 Note: The adjusted intraoperative (supine) target (A) results in the post-operative (standing) outcome, based on a 13° posterior tilt in standing relative to supine (negative is posterior). The calculator is available at http://billwalter.com.au/calculator/pelvic-tilt/
Note: The adjusted intraoperative (supine) target (A) results in the post-operative (standing) outcome, based on a 13° posterior tilt in standing relative to supine (negative is posterior). The calculator is available at http://billwalter.com.au/calculator/pelvic-tilt/
The question is then whether this adjusted target is a viable solution for the entire patient population. The answer is yes. Using the 39°/16° intraoperative target and the estimated distributions in Figure 4, the pelvic tilts that result in ±10° post-operative anteversion are -18.7° and 7.7°. Figure 8 highlights the portions of the patient population with supine-to-standing tilts less than -18.7° or greater than 7.7°. The areas are so small that they are barely discernible. In fact, using the adjusted target, an estimated 0.3% of the population would have an absolute change in anteversion greater than 10°.
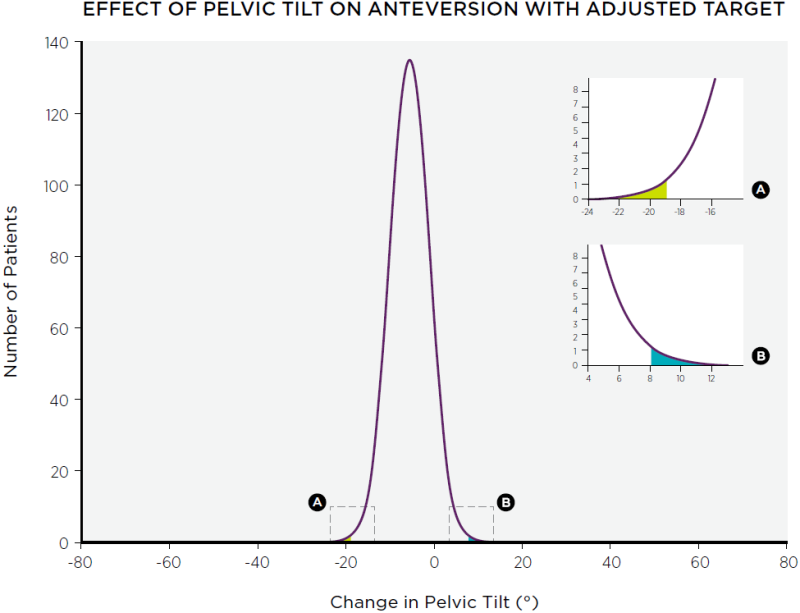
Note: Green and blue areas indicate patients with ≥10° change in anteversion due to pelvic tilt of ≤-18.7° or ≥7.7°, respectively.
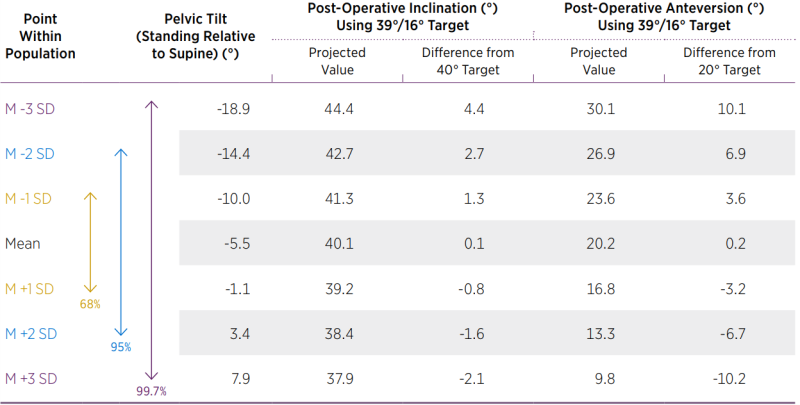
The adjusted (39°/16°) intraoperative target also leads to post-operative inclination angles that are projected to be well within ± 10° of the target. Using a standard deviation of 4.45° 2, the projected post-operative acetabular cup orientation was calculated at 1, 2, and 3 standard deviations from the mean. Shown in Table 1, the post-operative inclination angles from 37.9° to 44.4° are within 3 standard deviations of the mean. For a normal distribution, 99.7% of the data are within ± 3 standard deviations from the mean. Therefore, almost all of the inclination angles are within ± 5° of the inclination target.
The Navbit Sprint system uses an inertial navigation system and a novel method of registration of the patient which does not rely on anatomical landmarks.
Read more